Pectoralis tears are a dramatic injury that can occur during heavy bench presses, explosive pushing movements, or a fall onto an outstretched arm. The pectoralis major muscle helps bring the arm across the chest and rotate inward, stabilizing the shoulder during pushing tasks. A tear can range from a small strain to a full-thickness rupture. Understanding what they are, their treatment and recovery is essential for athletes and active individuals aiming to return to sport safely.
What is a pectoralis tear?
Most tears involve the tendon at the humeral insertion or the muscle belly near the sternum. The injury often results from a sudden, forceful push or a resisted eccentric load when the arm is extended and externally rotated. Athletes in weightlifting, football, basketball, and other high-demand sports may be at higher risk, especially when fatigued or attempting heavy loads. The severity of the tear—partial versus complete—strongly influences treatment decisions and timelines for recovery.
Signs, symptoms, and diagnosis
Common warning signs include a sharp pop or tearing sensation in the chest, immediate weakness during arm adduction or push movements, visible deformity in some cases, and bruising that develops over days. A clinician will assess strength, range of motion, and functional capacity, then typically order imaging such as an MRI to determine whether the tear is in the tendon, muscle, or both and to gauge retraction and tissue quality. Early and accurate diagnosis helps tailor a safe and effective treatment plan.
Treatment options
Treatment depends on the tear’s size, location, severity, and the patient’s goals. Non-surgical management can be appropriate for partial tears or individuals with lower functional demands. It usually includes rest followed by a structured rehabilitation program, pain control, and gradual loading to restore range of motion and strength. In some cases, immobilization for a short period may be advised, followed by progressive exercises focusing on eccentric control and scapular stability.
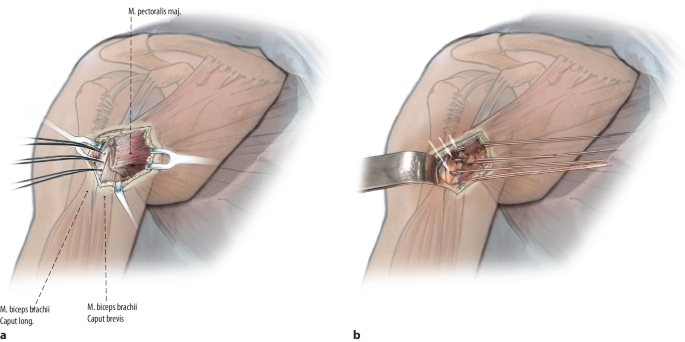
Surgical repair is often considered for complete tears, high-grade ruptures, or athletes who require maximal strength and rapid return to high-load activities. Surgery generally aims to reattach the tendon to its insertion or repair the torn muscle fibers, followed by a supervised rehabilitation protocol. The decision between non-surgical and surgical treatment is individualized, weighing the potential for full recovery against the risks and recovery timeline.
Recovery and rehabilitation
Recovery varies with tear type and treatment choice. Non-surgical rehab typically spans several weeks to months, emphasizing gradual range-of-motion restoration, controlled strengthening, and sport-specific conditioning. Return to unrestricted activities may take 3–6 months for mild cases and longer for more extensive injuries.
Post-surgical rehabilitation is more structured and often longer, typically involving immobilization for several weeks, followed by a progressive program that rebuilds tendon strength, tendon-to-bone healing, and full muscular control. Athletes may require 6–12 months before returning to high-speed, high-load activities. A gradual, criteria-based progression—based on strength symmetry, pain-free motion, and functional testing—helps minimize reinjury risk.
Return to sport and prevention
Returning to sport should be guided by objective milestones rather than elapsed time alone. Criteria commonly include pain-free movement, symmetrical shoulder and chest strength, and successful completion of sport-specific drills. Prevention strategies focus on proper warm-ups, gradual load progression, balanced chest and back training, and attention to technique during pushing movements. Eccentric strengthening and progressive overload, when applied carefully, may reduce the likelihood of future tears.
For deeper dive into this topic, what are pectoralis tears their treatment and recovery.
Additional resources can be found on the Veriibe homepage for broader guidance on sports injuries, rehabilitation, and return-to-play strategies.